Vascular diseases
Multiple and sometimes severe and life-threatening vascular diseases can effectively and minimally invasively be treated by interventional radiological methods.
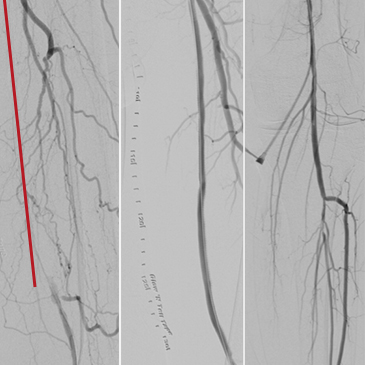
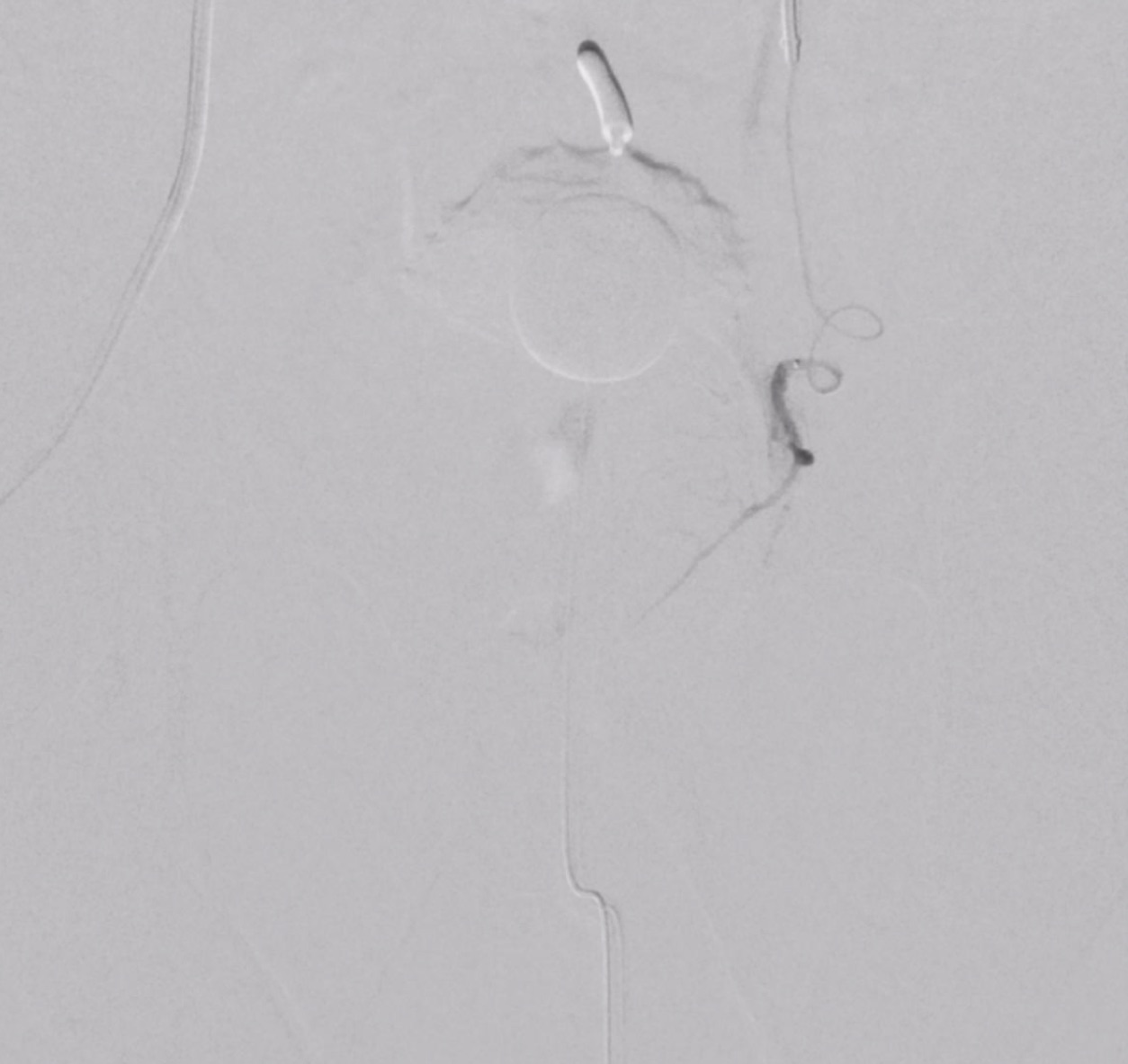
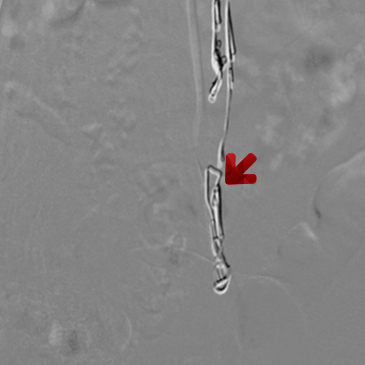
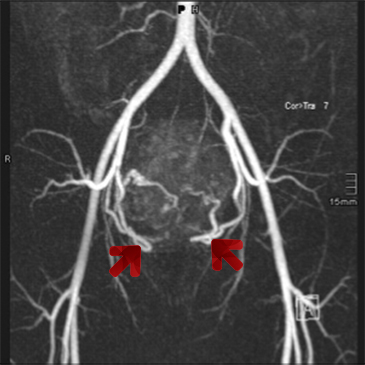
PAOD (=peripheral arterial occlusive disease) as well as occlusive disease in other arterial areas like the visceral, the subclavian, and carotid arteries, are the most common types of vascular diseases that can be treated in a minimally invasive manner.
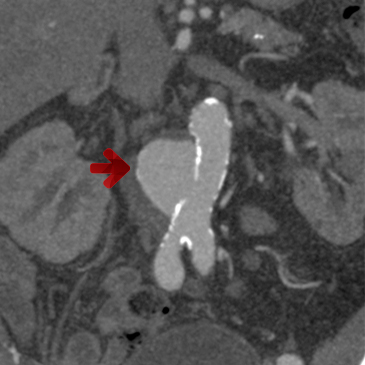
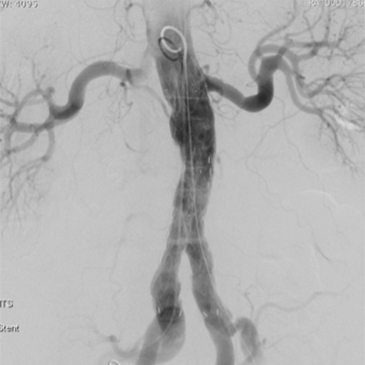
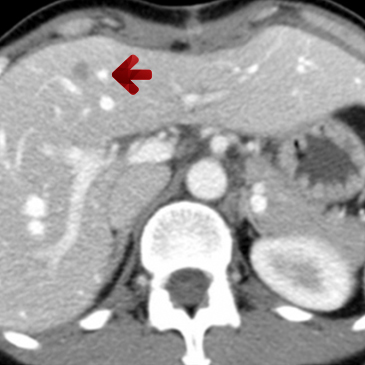
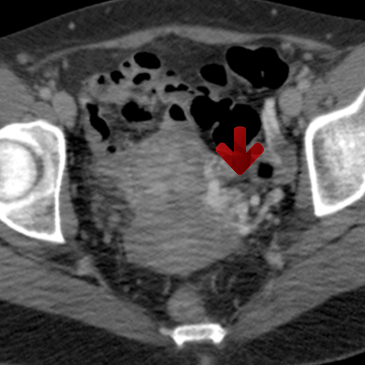
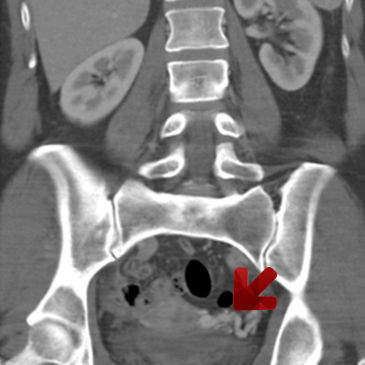
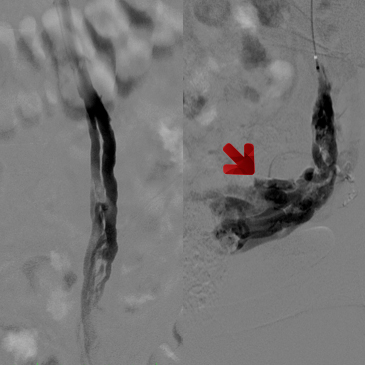
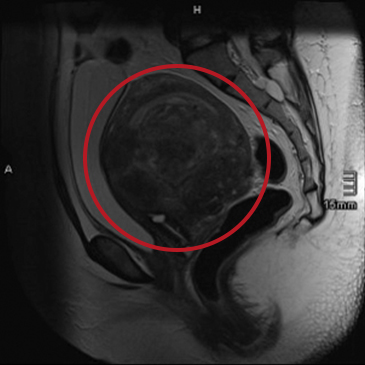
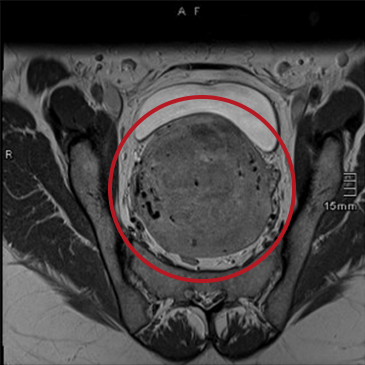
Another very important target for interventional radiology are the diseases of the thoracic and abdominal aorta, and, in particular, the pathological widening of these large vessels (aneurysms). Together with our surgical partners, interventional radiology is also able to treat these diseases highly effectively with minimally invasive methods.